
Severe asthma biologic injections, such as tezepelumab, offer a shift away from oral corticosteroids and a path to clinical remission for patients by targeting underlying inflammation. However, real-world evidence is essential in understanding effectiveness, safety and predictors of response to truly move towards precision medicine in the severe asthma population, as consultant respiratory pharmacist Lynn Elsey explains.
Over the last decade the treatment of severe asthma has rapidly changed due to an increased understanding of the heterogeneity and immunopathogenesis of the disease.1,2 The better understanding of asthma phenotypes, which can be identified through biomarkers, has shifted the focus of treatment to a personalised and targeted approach through biologic treatments.
Currently, the available biologics target immunoglobulin E, interleukin-5 and its receptor, interleukin-4 receptor, and thymic stromal lymphopoietin (TSLP). The evidence from randomised controlled trials of the biologics has demonstrated their effectiveness in reducing asthma exacerbations, healthcare resource utilisation, and maintenance and oral corticosteroid dependence, as well as improving quality of life.2
However, the limited patient populations and controlled environments of clinical trials do not always provide a clear understanding of how the patient population will respond in the real world.3,4
In the UK, severe asthma services adopt a multidisciplinary approach that provides specialised assessment and treatment for individuals with severe asthma. Eligibility for the severe asthma biologics is outlined in the National Institute of Health and Care Excellence (NICE) technology appraisal guidelines.
The eligibility criteria in the NICE guidelines – for example, for tezepelumab – were created from reviews of the clinical and cost-effectiveness data based on clinical trial findings and may not reflect patients’ response in the real-world setting.5 Currently, there is a lack of a clinical algorithm to identify the right biologic for the right patient.
Once initiated on biologics, patients must undergo an annual review to ensure they have responded with clinical improvement and significant reduction in oral corticosteroids.
Benefits of RWE for severe asthma biologics
Real-world evidence (RWE) for severe asthma biologics provides an understanding of the actual safety and effectiveness of the specific drugs in patients. This is vital to target the right drugs to the right patients.
Combining evidence from clinical trials with RWE has provided an understanding of predictors of response and the impact that other factors such as smoking, inhaler adherence or comorbidities can have on the patient’s response.3
Selecting the correct severe asthma biologic requires careful consideration of the mechanism of action of the biologics, the patient’s phenotype and associated comorbidities, but with increasing biologics available, treatment decisions can be difficult.3 RWE can guide treatment selection and personalise treatment choice.
The latest biologic to be approved in the UK is tezepelumab. It is the first TSLP blocker monoclonal antibody licensed for the treatment of severe asthma.
Clinical trials of tezepelumab versus placebo demonstrated greater reduction in risk of an exacerbation (0.93 (n=528) vs 2.1 (n=531); RR=0.44; 95% CI: 0.37–0.53; P<0.001); reduction in hospitalisation (0.06 (n=528) vs 0.27 (n=531); RR=0.21; 95% CI:0.12–0.37); improved lung function, with a 230ml improvement with tezepelumab at week 52 compared with baseline versus 100ml for placebo (95% CI: 0.08–0.18; P<0.001); and improved quality of life with tezepelumab.6–9
However, little is known about real world safety and efficacy, including which patient groups will demonstrate the greatest clinical benefit, which is especially important with tezepelumab as there are no biomarker or phenotypic restrictions.4,6
Real-world efficacy of tezepelumab
Manchester University NHS Foundation Trust provides specialist severe asthma multidisciplinary care and biologics across three hospital sites. Collaboration across the centres enables collation of real-world outcomes to broaden understanding of predictors of response and improve the ability to personalise care.
The latest retrospective review of the real-world efficacy of tezepelumab patients (n=55) found significant improvements in asthma control, quality of life, fractional exhaled nitric oxide (FeNO), and oral corticosteroid and antibiotic exposure in responders after 12 months of treatment (see Figure 1). This aligns with the clinical trial data.
Treatment was stopped in year one in 29% of patients due to side effects including palpitations, joint pain, fatigue, headaches, hives, rashes and gastric side effects (n=7), as well as increased symptoms and exacerbations (n=8) and death (n=1).
The comprehensive collection of clinical outcomes, previous biologic exposure, biomarkers and modifiable factors such as inhaler adherence, body mass index and smoking status enabled the analysis of differences between responders and non-responders, however no significant difference could be identified between the groups due to the limited sample size.10
This has prompted a future larger study to further examine predictors of response and drivers of non-response. In addition, identification of a cohort of non-responders who failed to significantly wean their maintenance steroid dose highlighted the need for a more comprehensive support programme for steroid wean.
Figure 1: Box and whisker plot showing changes in clinical outcomes over 12 months of tezepelumab treatment10
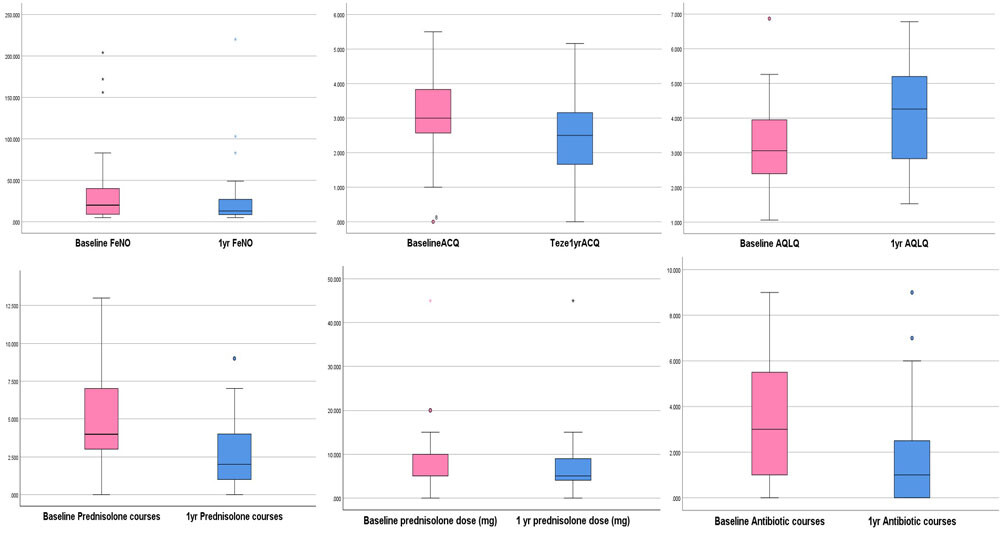
Clinical outcomes: FeNO (ppb), asthma control questionnaire (ACQ), asthma quality of life questionnaire (AQLQ), maintenance prednisolone dose (mg), antibiotic courses and exacerbations.
Severe asthma biologics and personalised care
It is estimated that 25% of patients will not respond to severe asthma biologics.11 Therefore, it is essential to utilise RWE to improve treatment selection and monitor response.
The Manchester study identified treatment cessation due to side effects ranging from common adverse effects of joint pain and headache to non-listed side effects including palpitations.10
These new adverse events could reflect an emerging real-world safety profile. However, they could be related to the nocebo effect – a recognised effect that can occur when a patient’s expectations for a treatment cause the treatment to have a worse effect than it otherwise would have.12
Tezepelumab’s patient information includes a few cautions including one related to cardiac events.6 This is due to a small number of cardiac events that occurred incidentally in patients during the clinical trial.6 Understanding that this could potentially impact a patient’s response to treatment highlights the need for effective patient counselling to increase their understanding and alleviate fear.
Asthma biologics are immunomodulators rather than immunosuppressants.13 However, there is a theoretical risk that blocking TSLP may increase the risk of serious infections.6
The clinical trials of tezepelumab against placebo did not demonstrate an increased rate of infection.7,8 A cohort of patients in our study ceased treatment in year one due to increased symptoms and infections. The nocebo effect may again have played a role, but a study of a larger patient population is required to further investigate if there is a link between tezepelumab and these reported infections.
Reassuringly, in those who responded to tezepelumab, there was a reduction in antibiotic courses. Potentially, antibiotic exposure could decrease due to a reduction in courses of oral steroids, which are often co-prescribed with antibiotics, or tezepelumab’s action on reducing mucus plugging.14
Severe asthma biologic injections and steroid reduction
Reducing exposure to oral corticosteroids through targeted immunomodulation is a main aim of biologics in severe asthma. Maintenance steroids could potentially mask asthma biomarkers, such as eosinophils and FeNO, and could impact patients’ eligibility for severe asthma biologics which require evidence of raised biomarkers.
Tezepelumab offers a treatment choice for this patient group, but the SOURCE study failed to show a significant improvement in oral corticosteroid dose reduction versus placebo in the overall population.15
In the Manchester real-world population, a group of 11 non-responders failed to wean their maintenance steroids in the first year. Further examination of this group is required to understand their dependence on oral corticosteroids.
This could be related to modifiable factors such as smoking and obesity. When these factors are adequately modulated, it could lead to a significant reduction of maintenance oral corticosteroids.
Failure to wean could also be related to adrenal suppression and monitoring for adrenal suppression is essential. Psychological dependence on steroids could be another factor, hence the need for access to clinical psychology to support this cohort.
It is important to also recognise that steroid withdrawal syndrome – an objective syndrome with symptoms including fever, anorexia, nausea, arthralgias and lethargy – could occur in patients who do not have biochemical evidence of adrenal suppression.16–18 These symptoms can significantly affect a patient’s belief in the treatment plan.
Successful steroid withdrawal requires a comprehensive and personalised multidisciplinary approach, including physiotherapists, psychologists, dieticians and pharmacists, to tackle modifiable factors, reduce anxiety and safely monitor withdrawal.17
Conclusion
The world of severe asthma treatment has been revolutionised by the introduction of targeted biologic treatments. To date, the RWE for severe asthma biologics demonstrates that combining targeted treatments with personalised multidisciplinary care can improve asthma outcomes and reduce the risks of long-term oral corticosteroid exposure.
A collaborative approach utilising the national and international patient registries and severe asthma networks to broaden our understanding of real-world efficacy and safety could potentially lead to a clinical algorithm to predict response. This would be a further step towards truly personalised care.
Author
Lynn Elsey
Consultant respiratory pharmacist, Manchester University NHS Foundation Trust
References
1 Orlovic M et al. Environmental, healthcare and societal impacts of asthma: a UK model-based assessment. ERJ Open Res 2024;10:00577-2023.
2 Gyawali B et al. Biologics in severe asthma: a state-of-the-art review. Eur Respir Rev 2025;34:240088.
3 Paoletti G et al. Biologics in severe asthma: the role of real world evidence from registries. Eur Respir Rev 2022;31:210278.
4 Lee Y et al. Roles of real-world evidence in severe asthma treatment: challenges and opportunities. ERJ Open Res 2023;9(2):00248-2022.
5 National Institute for Health and Care Excellence. Tezepelumab for treating severe asthma. Technology appraisal guidance TA880. 2023 [Accessed November 2025].
6 Electronic Medicines Compendium. Tezspire (tezepelumab). Summary of Product Characteristics. 2022 [Accessed November 2025].
7 Menzies-Gow A et al. Tezepelumab in adults and adolescents with severe, uncontrolled asthma. N Engl J Med 2021;384(19):1800–9.
8 Corren J et al. Tezepelumab in adults with uncontrolled asthma. N Engl J Med 2017;377(10):936–46.
9 Corren J et al. Efficacy of tezepelumab in patients with severe, uncontrolled asthma: a pooled analysis of the phase 2b PATHWAY and phase 3 NAVIGATOR studies. Poster presented at: AAAAI 2022 (Poster 044).
10 Elsey L et al. Real world one-year outcomes for severe asthma patients on tezepelumab. Poster presented at: Eur Resp Soc Congress, Amsterdam, 2025.
11 Hansen S et al. Clinical response and remission in patients with severe asthma treated with biologic therapies. CHEST 2024;165(2):253–66.
12 Grosso F et al. Risk factors associated with nocebo effects: A review of reviews. Brain Behav Immun Health 2024;38:100800.
13 Dorscheid D et al. Guidance for administering biologics for severe asthma and allergic conditions.
14 Nordenmark LH et al. Tezepelumab and mucus plugs in patients with moderate-to-severe asthma. NEJM Evid 2023;2(10):EVIDoa2300135.
15 Weschler M et al. Evaluation of the oral corticosteroid-sparing effect of tezepelumab in adults with oral corticosteroid-dependent asthma (SOURCE): a randomised, placebo-controlled, phase 3 study. Lancet Respir Med 2022 Jul;10(7):650–60.
16 Aung H et al. Assessment of an Oral Corticosteroid Withdrawal Pathway for Severe Asthma Patients Receiving Biologic Therapies. J Allergy Clin Immunol Pract 2025;13(7):1807–15.e4.
17 Calzetta L et al. Oral Corticosteroids Dependence and Biologic Drugs in Severe Asthma: Myths or Facts? A Systematic Review of Real-World Evidence. Int J Mol Sci 2021;22:7132.
18 Margolin L et al. The steroid withdrawal syndrome: A review of the implications, etiology, and treatments. J Pain Symptom Manage 2007;33:224–8.