
Despite a marked reduction in referral rejections since the introduction of the NHS Discharge Medicines Service five years ago, a significant number of referrals continue to be rejected or left unactioned. This retrospective study explores the reasons behind these missed opportunities and highlights areas for improvement across hospital and community pharmacy services.
When people transfer between different care providers, such as at hospital admission or discharge, there is a risk of poor communication, medication discrepancies, adverse drug events, avoidable hospital readmissions and increased healthcare costs.1,2 What’s more, this process of discharge from the hospital back to primary care can leave patients confused about their medication.
The extent to which a patient’s medication may change from admission to discharge has been well documented.3,4 National evidence estimates that around 1.8 million medication errors occur annually at transitions of care in England, with approximately 44% occurring at discharge.5
Ideally, medication changes made during a hospital stay should be explained to the patient, documented and then communicated to the next healthcare provider involved in their care. After leaving the hospital, GPs are expected to check and update the individual’s medication list as soon as possible, but various barriers may prevent this.6
Launch of the discharge medicines service
Pharmacists in hospitals, primary care and the community are all involved in preventing harm, reducing readmissions and improving outcomes at transitions of care.7
The discharge medicines service (DMS) was launched in England in February 2021 as an essential service for community pharmacy contractors. During the transition of care, hospital teams refer patients to their regular community pharmacy and provide all the relevant information about medication changes made during their hospital stay.
Operationally, the DMS involves three stages: community pharmacies clinically review the referral within 72 hours, check that the first post-discharge prescription issued by the patient’s GP aligns with the discharge plan, and counsel the patient or their carer to ensure their new medication regimen is properly understood.
Transfer of care and medicines
Prior to the launch of the DMS, Royal Cornwall Hospitals NHS Trust (RCHT) was involved in the transfer of care around medicines (TCAM) service.
By using PharmOutcomes as a secure electronic referral platform, the Trust was able to electronically transmit discharge information from the hospital pharmacy to a specific community pharmacy at the time of patient discharge.8
This TCAM service involved referrals only to community pharmacies in Cornwall, whereas the NHS England-commissioned DMS takes this one step further and enables referrals to the patient’s regular pharmacy regardless of its location in England.
As part of the TCAM service, and now the DMS, community pharmacies have the option on PharmOutcomes to either ‘accept’ or ‘reject’ the referral sent from the hospital.9 As such, if a community pharmacy neither acknowledges the referral nor registers that any action has been taken, the referral status remains recorded as ‘Referred (no action)’ in the system.
According to the NHS England Medicines Safety Improvement Programme, available via NHS Futures and based on an observational study of the TCAM service,10 the DMS will prevent one readmission for every 10 community pharmacy consultations.
Hence, rejected and unactioned referrals represent a potential patient safety gap. In collaboration with relevant stakeholders, there may be opportunities to reduce the frequency of these, which is what our recent study aimed to address.
DMS study aims and methods
Our retrospective study analysed PharmOutcomes data covering four years of the TCAM service and five years of DMS activity to determine how the proportion of referrals rejected by RCHT has changed over this nine-year period.
The datasets were used to quantify referral and rejection rates across the study period, while the DMS data were further examined to categorise the reasons for referral rejection and to assess whether these factors could be mitigated.
Anonymised data were downloaded in early February 2026, then collated, analysed and summarised in Microsoft Excel by a pharmacist at the hospital who routinely worked with this dataset.
As this project falls within the definition of a service evaluation, formal ethical approval was not required under the UK NHS Research Ethics Committees’ guidance. It was registered a priori with the RCHT Clinical Effectiveness Unit as a service evaluation.
DMS referral rejection results
During the TCAM service from 18 January 2017 to 20 February 2021, there were 16,326 referrals, of which 5,800 were rejected – equating to a rejection rate of 36%. A further 2,600 (16%) TCAM service referrals were recorded as ‘no action’.
During the DMS period from 22 February 2021 to 31 December 2025, there were 3,283 rejections from 40,259 referrals, with a mean rejection rate of 8%, but in 2025 it fell to 5%, as shown in Figure 1. There were also 7,051 DMS referrals (18%) recorded as no action.
Figure 1. Number of DMS rejections, total referrals and percentage of referrals that were rejections
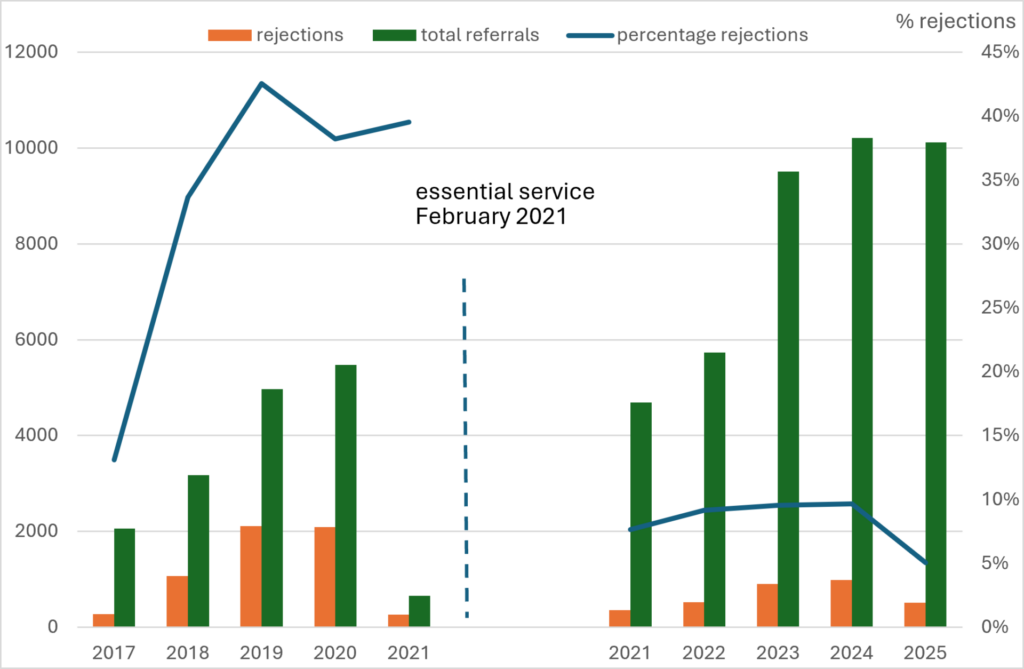
Under the TCAM service, the mean age of patients with rejected referrals was 72 years (range 3 to 105 years), and 46% of 5,800 rejections were for males. Under the DMS, the mean age of patients with rejected referrals was 69 years (range 1 to 101), and 47% of 3,283 rejections were for males.
Of the 3,283 DMS rejections, 325 unique community pharmacies were responsible for them. However, rejection activity was concentrated among a relatively small number of community pharmacies, with 12 (all in Cornwall) accounting for 52% of the rejections (ranging from 61 to 303 rejections over the five years).
The rejection rate for community pharmacies situated outside of Cornwall, including online pharmacies, was 8% (286 of 3,563 total referrals) – the same as that for pharmacies located in Cornwall (2,997 of 36,696 total referrals).
A free-text entry describing a reason for the rejection was available for 3,197 (97%) of the 3,283 rejections. The broad themes of reasons for rejections are shown in Table 1.
Table 1. Reasons for DMS rejections by main themes and possible source of process failure
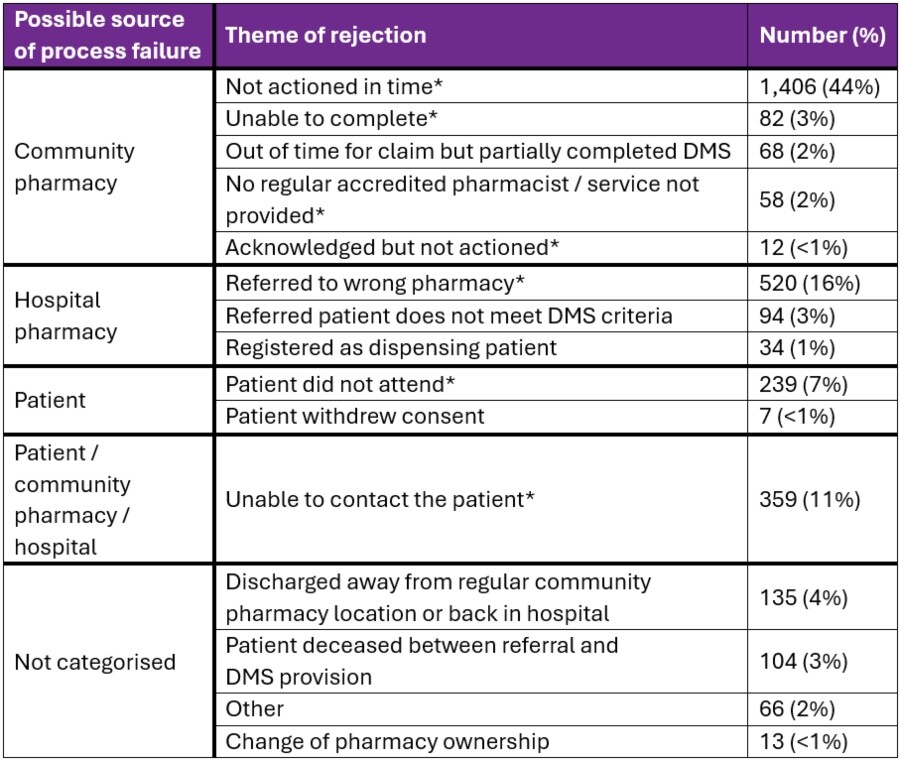
* Potentially avoidable
Study limitations
The retrospective nature of data collection limits this work, and the subjective categorisation of rejection reasons into main themes may have misinterpreted the free text entry. For example, the community pharmacy may have listed ‘unable to contact patient’ as a primary reason, even if the patient had been discharged away from their usual home setting.
The scope of our study was also limited to a single hospital-based DMS, which may restrict transferability to other settings.
Furthermore, we have not analysed whether there is any relationship between the rejection rate at individual community pharmacies and the provision of other pharmacy services.
Avoiding DMS rejections
In this five-year retrospective study focusing solely on rejected DMS referrals, we estimate that up to 82% of 3,197 rejections were potentially avoidable. In addition, we show a decrease in the mean rejection rate from the TCAM service to the DMS, from 36% to 8%.
This work builds on our previous report examining DMS rejections over the 12-month period to April 2023.9 In both papers, we acknowledged that any community pharmacy activity under the TCAM service was voluntary, as no contractual or service reimbursement arrangements were made. In contrast, the community pharmacy receives funding for DMS delivery as an essential service. Others have reported, albeit from a small-scale study of 158 DMS referrals, a similar rejection rate of 7.59%.11
Over half of the potentially avoidable rejections in our study (57%) were considered process failures at the community pharmacy, such as not actioning referrals in time or not having a regular accredited pharmacist.
Interestingly, a recent report examining the Pharmacy First service and other community pharmacy activity noted that in recent years, there are fewer pharmacies open for fewer hours, yet they are dispensing more prescriptions and providing more services within that condensed period.12
It concludes that the present pace of growth in workload is not sustainable and that extra workforce and better premises capacity are a necessity.12 Consequently, there needs to be work at a national level on how to support community pharmacies struggling with staffing issues or lack of time to undertake the DMS.
Future work should also be undertaken with the hospital pharmacy team to improve the accuracy of community pharmacy selection for the referral. For instance, all patients should be asked to identify their regular pharmacy, rather than the hospital pharmacy team assuming any prior record of the regular community pharmacy is correct. Alternatively, utilising the NHS Organisation Data Service search function can assist in correctly identifying the nominated community pharmacy.
The DMS patient experience and communication
An inability to contact the patient was selected as the reason for 359 rejections. As others have noted, the specific reasons for this need to be explored further.10
However, possible reasons include issues with service design and delivery, such as patients not answering calls from unidentifiable numbers, or errors in the hospital patient administration system from which the patient contact details are derived, rather than the patient consciously refusing a referral.
There may be an option for community pharmacies to use alternative contact methods, such as text messaging, to support engagement after discharge.
Although we have categorised patients who did not attend the community pharmacy for stage 3 of the DMS as potentially avoidable, there may be a variety of undocumented and unknown reasons for this.
These include the patient experiencing transport barriers, their perception that there was no substantial change in medication during the hospital admission, or their lack of understanding of the purpose of the DMS referral. It should be noted, however, that a leaflet about the service is provided to patients receiving medication at discharge.
The communication gap between hospital teams and community healthcare providers at discharge can also lead to delays in care, confusion and drug-related problems in the community, particularly when patients are discharged with complex medication regimens.13
It is recognised that when community pharmacists receive a discharge medication list, they play a key role in medication management and in addressing drug-related problems after hospital discharge.14
As regards the DMS, others have estimated the significant potential to reduce readmissions of patients owing to medicines-related issues, using outcome measures from the TCAM service and the Welsh DMS.15
However, to our knowledge, there has been no formal evaluation of the impact of the English DMS on patient benefit. In this context, we recognise the uncertainties surrounding our estimate of 267 preventable readmissions over five years, had the avoidable rejections actually been acted upon.
Furthermore, with a total rejection rate of 8% for all referrals and yet a ‘Referred (no action)’ rate of 18%, perhaps more effort should be directed at understanding why some referrals are simply not acknowledged and actioned on PharmOutcomes by community pharmacies.
Conclusion
Community and hospital pharmacists, and organisational leaders, still need to work together cohesively if the potential benefits of DMS are to be more widely realised across health settings.
Although referral rejection rates have fallen since the transition from TCAM to DMS, a significant proportion of referrals continue to be rejected or remain unactioned. Many of the reasons identified in this study appear to be potentially avoidable, suggesting opportunities to strengthen referral processes, improve communication between care settings and support more consistent service delivery.
Further work is needed to understand and address the factors contributing to both rejected and unactioned referrals.
Authors
Michael Wilcock FRCPharm
Head of the prescribing support unit, Pharmacy Department, Royal Cornwall Hospitals NHS Trust, UK
Liam Bastian MRCPharm
Chief pharmacy information officer, Pharmacy Department, Royal Cornwall Hospitals NHS Trust, UK
Amanda Fidelis MPharm
Senior pharmacist and community pharmacy clinical lead, Medicines Optimisation Team, Cornwall & Isles of Scilly Integrated Care Board, UK
References
1 Linkens AEMJH et al. Medication-related hospital admissions and readmissions in older patients: an overview of literature. Int J Clin Pharm 2020;42:1243–51.
2 Alqenae FA, Steinke D, Keers RN. Prevalence and nature of medication errors and medication-related harm following discharge from hospital to community settings: a systematic review. Drug Saf 2020;43:517–37.
3 World Health Organization. Medication safety in transitions of care. 2019.
4 Himmel W et al. Drug changes at the interface between primary and secondary care. Int J Clin Pharmacol Ther 2004;42:103–9.
5 Camacho EM et al. Estimating the impact on patient safety of enabling the digital transfer of patients’ prescription information in the English NHS. BMJ Qual Saf 2024;33:726–37.
6 Klepacz N et al. General practice follow-up after hospital discharge in older adults: Retrospective records analysis. Br J Gen Pract 2026 Apr 2;BJGP.2025.0627.
7 Zavaleta-Monestel E et al. Transitions of care: integrating pharmacists to prevent harm worldwide. Eur J Hosp Pharm 2025;ejhpharm-2025-004784.
8 Health Innovation West of England. Transitions of care around medicines (TCAM). Available at www.healthinnowest.net/our-work/transforming-services-and-systems/medicines-optimisation/transfers-of-care-around-medicines/ [Accessed June 2026].
9 Wilcock M et al. Community pharmacy discharge medicines service activity as recorded in PharmOutcomes: a retrospective exploration and analysis. Int J Pharm Pract 2024;32:274–9.
10 Nazar H et al. New transfer of care initiative of electronic referral from hospital to community pharmacy in England: a formative service evaluation. BMJ Open 2016;6:e012532.
11 Hall M et al. Discharge medicines service (DMS). A tertiary specialist paediatric hospital’s experience. BMJ Paed Open 2025;9(Suppl 2):A41–A42.
12 The Pharmacists’ Defence Association. With 25% growth in the Pharmacy First service, has England’s community pharmacy reached total system capacity? PDA; 2026.
13 Grandchamp S et al. Pharmaceutical interventions on hospital discharge prescriptions: prospective observational study highlighting challenges for community pharmacists. Drugs Real World Outcomes 2022;9(2):253–61.
14 Johnstone KJR et al. Bridging the Gap: Systematic Review of Strategies to Facilitate Post-Discharge Continuity of In-Hospital Medication Changes in Older Adults. Drugs Aging 2026;43:137–52.
15 Thayer N, Mackridge AJ, White S. Predicting the potential value of the new discharge medicines service in England. J Pharm Health Serv Res 2023;14:248–55.